Joint consideration of LDL-C and polygenic risk for incident coronary heart disease in a multi-ethnic cohort of 48,881 individuals
European Journal of Preventive Cardiology


Abstract
Elevated concentrations of LDL-cholesterol (LDL-C) are a major independent modifiable risk factor for coronary heart disease (CHD). However, the degree to which background polygenic risk can modulate the effect of high LDL-C remains unclear.
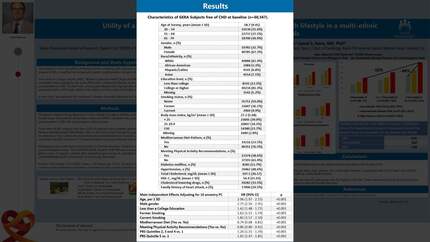
We utilized data from a subset of the Genetic Epidemiology Resource in Adult Health and Aging (GERA) multi-ethnic cohort (n=48,881; mean ± SD age = 58.1 ± 10.3 years; 63% female; 18% non-European ancestry) who were non-diabetic and not taking cholesterol lowering medication at baseline in 2003-2007. We stratified the cohort into three groups of CHD genetic risk (low=quintile 1; intermediate=quintiles 2, 3 and 4; and high=quintile 5) using a 12-SNP Polygenic Risk Score (PRS) for CHD (CARDIO inCode-Score, GENinCode Plc). Incident CHD consisted of primary in-patient codes for angina pectoris, myocardial infarction, revascularization procedures or CHD death through 12/31/2022 (n=1,725); mean follow-up was 14.3 years. Age-adjusted CHD rates per 10,000 person-years were estimated using Poisson regression (accounting for death and health plan disenrollment) according to polygenic risk and LDL-C level. Hazard ratios and 95% confidence intervals for 1 standard deviation (SD) increment of LDL-C in each PRS group were obtain using Cox regression adjusting for 10 principal components of ancestry plus traditional risk factors. We tested for formal interaction LDL-C*PRS as continuous variables in the fully adjusted model. As a complimentary approach we tested interaction between high PRS (quintile 5 vs. lower) and LDL ≥190 (vs lower). Finally, we calculated number needed treat (NNT) to prevent 1 CHD event in each PRS group.
After multivariate adjustment, each 1 SD increment of LDL-C was associated with 1.07 (95% CI, 0.95-1.21; p=0.24), 1.22 (95% CI, 1.15-1.29; p=0<0.0001) and 1.14 (95% CI, 1.03-1.26; p=0.009) increased hazard of CHD among low, intermediate, and high PRS groups, respectively. There was no interaction between linear effects of LDL-C and PRS (p=0.34). On the other hand, we found evidence of interaction (p=0.002) between high PRS and LDL ≥ 190. The NNT was lowest in the high PRS group and highest in the low PRS group (see Figure below).
Our results are consistent with a multiplicative model of high polygenic risk and high LDL on CHD risk. While all patients with elevated LDL-C ought to be treated, our data suggest that an earlier and more aggressive lipid lowering therapy may be directed towards those with high polygenic risk. Figure.
Contributors



You may be interested in