Reservoir-excess pressure analysis, aiding critical care management by revealing subtle changes in vasomotor status, is closely linked to dicrotic notch morphology
European Heart Journal - Acute CardioVascular Care


Abstract
Haemodynamic(HD) monitoring is a vital element of critical care and currently mainly controlled by mean arterial pressure(MAP). But even when recommended MAP is achieved, there is still a significant risk of compromised HD. Reservoir-excess pressure analysis(REPA) offers valuable information beyond standard arterial blood pressure(ABP) parameters, including reservoir pressure(Pres) as a Windkessel-like buffering capacity of elastic large arteries and diastolic rate constant(DRC) as a measure of peripheral vasotonus. In addition, dicrotic notch morphology can theoretically provide information on preload, contractility and afterload status.
We examined if HD monitoring can be advanced together with REPA parameters and if dicrotic notch morphology of peripheral ABP waveforms can provide an instantaneous information on peripheral arterial Pres status.
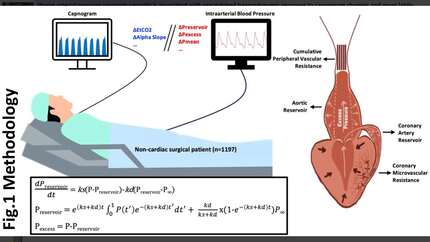
Intra-ABP signals from 576 vessels in 288 unique non-DM/HT patients undergoing non-cardiac surgery were analysed. For each patient, two signal windows of min and max mean ABP intervals were auto-detected and averaged to extract parameters. Pres waveform was transformed further using diastolic pressure subtraction (Pres(rel) and INTPRES(rel)). Arterial reservoir capacity(ARC) was defined as Pres(rel)mean/Pexcmean. Dawber classification was visually performed based on previous definition. Amplitude index(AI) defined as diastolic wave peak(DWP)/systolic blood pressure(SBP). By definition, AI was calculated only for Dawber I&II (Fig. 2). Impact of different vasoactive drugs on REPA were evaluated.
Presence of a prominent dicrotic notch was associated with higher reservoir capacity and lower DRC(p<.001)(Fig 1a). Higher AI was present with higher INTPRES(r:0.454 p<.001), Presmean(r:0.308 p<.001), ARC(r:0.172 p<.001) and lower DRC(r:-0.357 p<.001)(Fig 1b). After vasopressor administration, a higher frequency of Dawber I&II was observed compared to baseline, while there was a tendency for class IV to disappear. Vasopressors improved Pres(p<0.05), in addition norepinephrine led to a slower DRC(p<.001). Conversely, nitroglycerin, a vasodilator, normalised systemic and local hyperperfusion(lowered Pexc)(p<.001). Different receptor interactions that differentiate HD effects on cardiovascular system (vasodilatory, vasoconstrictive and cardiac output effects) of vasoactive agents could be distinguished by REPA(Fig 1c).
Coexistence of attenuated vasotonus and absent dicrotic notch suggest that Dawber class may indicate impaired reservoir status. Moreover, the REPA parameters allowed the detection of subtle changes in the patients' HD status and differentiated the effect of vasoactive agents. Thus, close monitoring of REPA and dicrotic notch morphology has the potential to improve critical care monitoring by identifying medication needs, alerting the treating physician, and allowing appropriate vasoactive drug administration by individual REPA status to improve outcomes.
Contributors



You may be interested in