Determinants of changes in peak oxygen consumption in patients with new onset heart failure
European Heart Journal


Abstract
Patients with heart failure (HF) with reduced ejection fraction (HFrEF) have a high risk of mortality. Cardio-Pulmonary Exercise Test (CPET) assesses peak oxygen consumption (pVO2) which is considered a key predictor of mortality and morbidity in patients with HFrEF. Factors responsible for the changes in pVO2 could consequently be of interest, as optimizing these factors may improve prognosis and overall quality of life in patients with HFrEF.
To investigate factors contributing to changes in pVO2 within a contemporary cohort of new-onset patients with HFrEF.
From December 2022 to September 2023, patients with new-onset HFrEF (European Society of Cardiology (ESC) criteria) were included from a HF outpatient clinic, who after referral to the clinic underwent 12 weeks of HF management according to ESC guidelines. This included physical training and optimization of pharmacological management of HFrEF. Baseline characteristics, CPET, medication and echocardiography were collected at referral and after 12 weeks. Changes in pVO2 were investigated according to baseline characteristics, changes in medication, and changes in echocardiographic parameters in both uni- and multivariable linear regression models. Significant independent variables were identified using stepwise selection (p<0.1), adjusted for age and sex. A p-value of 0.05 was considered significant.
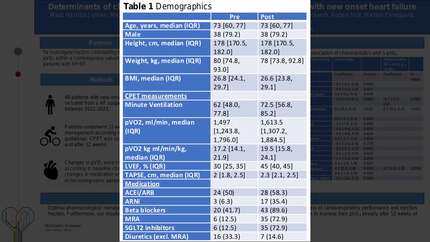
We included 48 patients with new-onset HFrEF with a median age of 73 (interquartile range (IQR): 60-77) years, 10 (20.8%) women, a baseline median left ventricular ejection fraction (LVEF) of 30% (IQR: 25-35), and a baseline median pVO2 of 17.3 ml/min/kg (IQR: 14.1-21.9). After 12 weeks, pVO2 improved with a mean of +2.18 ml/min/kg (95% confidence interval (CI) 1.25 to 3.10, p<0.01) and LVEF improved with a mean of +11.7% (95% CI 7.9 to 15.6, p<0.01). In univariable analyses increasing age were negatively associated with pVO2 changes (p=0.04) and increasing minute ventilation (MV) and initiation of sodium-glucose cotransporter (SGLT2) inhibitors were all positively associated with pVO2 changes (p<0.01 and p=0.03, respectively). Other clinical variables included in the analysis were not significantly associated with a change in pVO2. In the multivariable analysis, body mass index emerged as an independent variable negatively associated with pVO2 changes, and MV and initiation of SGLT2 inhibitors remained significantly positively associated with pVO2 changes.
Optimal pharmacological management and physical training in patients with new-onset HFrEF, induce a significant recovery of cardiorespiratory performance and ejection fraction. Furthermore, our results suggest that the initiation of SGLT2 inhibitors in patients with new-onset HFrEF appears to improve their pVO2 already after 12 weeks of optimal HF management. Baseline Associations
Contributors

M T Thunestvedt
Author
M L Lamberts
Author
M S Schou
Author
S N Nielsen
Author
M E Elmegaard
Author
N N Nouhravesh
Author
A H Holt
Author
C S Shurenberg
Author
You may be interested in