Prognostic value of left atrial strain for outcome of catheter ablation in patients with atrial fibrillation and moderately enlarged left atrium
European Heart Journal


Abstract
Atrial fibrillation catheter ablation (AFCA) is an effective rhythm control method for patients with AF, but AF recurrence is higher in patients with a large left atrium (LA). We explored whether pre-procedural LA strain has incremental prognostic value for the long-term rhythm outcomes of AFCA in patients with AF and moderately enlarged LA size (45≤LA diameter<50mm).
We included 2,269 patients who underwent de novo AF catheter ablation (men 72.2%, 59.1[±10.7] years, paroxysmal AF 64.0%). We divided grouped into 5 mm increments and determined the appropriate cut-off of LA diameter (45mm) predicting the difference in long-term rhythm outcome by the log-likelihood values of multivariate Cox proportional hazard models. Patients with moderately enlarged LA size (45≤LA diameter<50mm, n=413) with borderline rhythm outcomes were used for analysis.
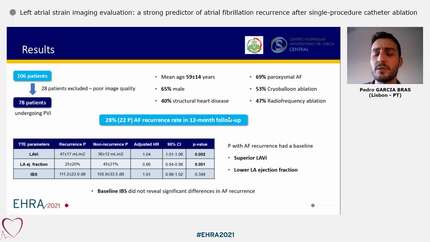
In the cohort of 413 patients who underwent AFCA with moderately enlarged LA size, AF was recurred in 208 patients (43.7%) after AFCA. We determined the appropriate cut-off of LA strain (12.5) predicting the difference in long-term rhythm outcome by the log-likelihood values of multivariate Cox proportional hazard models. During 24 months [10-50] follow-up, patients with low LA strain (<12.5) were showed worsen rhythm outcome than high LA strain (Log-rank p<0.001). Patients with AF recurrence after AFCA were independently associated with low LA strain (HR 1.539 [1.130-2.094], p=0.006), and paroxysmal AF (OR 0.651 [0.469-0.905], p=0.011). Furthermore, the likelihood ratio test demonstrated a significant influence of adding LA strain by TTE (χ2 = 13.90 [P < 0.001]).
LA strain using baseline echocardiography has a predictive power for AF recurrence after AFCA in patients with moderately enlarged LA size (45≤LA diameter<50mm).





You may be interested in