Feasibility and efficacy assessment of a novel size-adjustable cryoballoon for ablation of atrial fibrillation in a multicenter clinical setting
European Heart Journal


Abstract
The POLARx-FIT cryoballoon (CB) system introduces a unique feature, allowing the selection of two distinct balloon sizes within a single catheter. This innovation holds promise for treating larger pulmonary veins (PV), providing increased flexibility to achieve optimal occlusions. However, there is a scarcity of clinical data supporting its application in this context.
To compare the benefits and safety of the new POLARx-FIT system to those of the existing POLARx system currently in use for PV isolation (PVI) in patients with atrial fibrillation (AF).
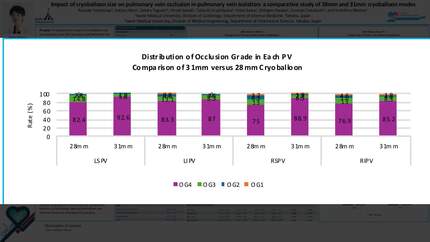
The first 140 consecutive patients who underwent CB-based PVI with the POLARx-FIT system were retrospectively compared with 300 consecutive patients treated with the POLARx system. Protocol-directed cryoablation was delivered for 180 sec or 240 sec according to operator’s preference for isolation achieved in ≤60 sec, or 240 sec if isolation occurred >60 sec or when time to isolation was not available. The ablation endpoint was PVI as assessed by entrance and exit block. In the POLARx-FIT group the choice of balloon size (28 or 31 mm) was determined during the procedure while attempting to occlude each vein.
Two-thousand one-hundred fifty-five cryo-applications (CBA) from 440 patients were analysed (300, 68.2% POLARx; 140, 31.8% POLARx-FIT). PVI was achieved with cryoablation only in all patients. The mean number of freeze applications per patient was similar between groups (5.0±1.4 in the POLARx-FIT vs 5.3±1.8 in the POLARx group, p=0.207) whereas the number of PVs treated in a single-shot fashion was higher in the POLARx-FIT group (444, 80.7% with one shot; 75, 13.7% with 2 shots; 31, 5.6% with more than 2 shots) than in the POLARx one (1168, 70.2% with one shot, p=0.0002; 294, 17.7% with two shots and 143, 8.6% with more than two shots). Among the POLARx-FIT cases, in 54.2% (n=298) of applications, the 31-mm diameter was employed as a first choice, while in the remaining 45.8% (n=252) of applications, the 28-mm diameter was adopted. A switch to a different balloon diameter was applied in 11.6% of cases. The first pass isolation (i.e. a single shot CBA to achieve PVI) was slightly higher when using a 31 mm diameter (n=250, 83.9%) than a 28 mm diameter (n=194, 77.0%, p=0.05). Three (0.7%) transient phrenic nerve palsy were observed (all in the POLARx group, 0.9%, p=0.554), with full recovery in the 48-h post procedure; no major procedure-related adverse events were reported at 30 days post-procedure.
In this first multicentric experience in a clinical practice setting, this novel cryo-balloon system proved to be safe and effective and resulted in a high proportion of successful single-freeze isolation. The intraprocedural flexibility of balloon size contributed to its versatility, leading to a variation in balloon diameter in about 12% of freeze applications.
Contributors

C Tondo
Author
G Pelargonio
Author
A Agresta
Author
M Schiavone
Author
R Ricciolino
Author
M L Narducci
Author
S Bianchi
Author
D Pecora
Author
M Cerini
Author
G Bencardino
Author
M Moltrasio
Author
C Albano
Author
A De Simone
Author
You may be interested in