Influence of a three-dimensional mapping system on acute safety and efficacy of pulsed-field ablation for atrial fibrillation
European Heart Journal


Abstract
Visualization of the multi-electrode pulsed-field ablation (PFA) catheter within a 3D-mapping system holds the potential to improve catheter maneuverability and enhance ablation outcomes, thereby improving procedural metrics.
The aim of our analysis, from a real-world nationwide registry, is to evaluate the impact of 3D-mapping system on acute safety and efficacy in the context of PFA of atrial fibrillation (AF).
All consecutive patients undergoing de novo AF ablation with the Farapulse system at 13 centers were included. Protocol-directed PVI was delivered using 2kV with 8 applications per vein, that is, 4 applications each in the basket and flower poses. Additional lesions were performed at the operator’s discretion. Procedures were stratified according to the use or not of 3D-mapping system to validate the lesions (MAP vs Standard).
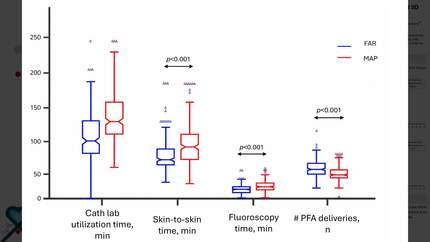
Among 1002 patients, 28.3% were females, 28.2% had persistent AF, mean age was 62.9±10 years, mean LVEF was 57.4±8%. A more extensive lesion set than PVI only (PVI plus) was performed in 230 (23.0%) of the cases. A 3D-mapping system was used to validate the lesion set in 201 (20.1%) of the cases, mostly when a more extensive lesion set was applied (40% in PVI plus vs 14.1% in PVI only, p<0.001). Four-thousand forty-five (99.1%) PVs were acutely isolated on first pass (26 patients with at least 1 PVs not isolated at first pass, 2.6%), as confirmed by both entrance/exit block and/or on subsequent 3D-mapping. No differences between MAP and Standard procedures were found in terms of first pass PVI (98.8% vs 99.1%, p=0.416) or number of patients with all PV isolated at first pass (95.5% vs 97.9%, p=0.079). At the end of the procedure PVI was achieved in all patients. By looking at procedural metrics, the total number of PFA deliveries (43±12 vs 39±10, p<0.0001) and PFA deliveries outside PVs (19.6±8 vs 15.1±6, p<0.0001) were higher in the MAP group, whereas the number of PFA deliveries to achieve PVI were lower (34±4 vs 36.4±7, p<0.0001). MAP procedures had longer skin-to-skin time (94[80-120]min vs 60[50-70]min, p<0.0001), time to PVI (20[15-27]min vs 18[14-24]min, p=0.0001) or fluoroscopy time (22[18-29]min vs 14[11-18]min, p<0.0001). The MAP group exhibited increased skin-to-skin time and fluoroscopy time, even when analyzing procedures separately for those involving PVI only and those involving PVI plus. Conversely, the total number of PFA deliveries to achieve PVI (53.8±8 vs 53.3±10, p=0.254) and time to PVI (17.5[14.5-22]min vs 18[12-25]min, p=0.516) were comparable between MAP and Standard groups during PVI plus. No major complications occurred in both groups.
In our real-life experience, the use of Farapulse PFA system for de novo AF ablation was rapid, safe and acutely effective resulting in a very high first-pass isolation rate. 3D-mapping system was used in a minority of patients and was not associated with an increase in acute success-rate.
Contributors

G Viola
Author
M Russo
Author
M Volpicelli
Author
B Stegagno
Author
S Bianchi
Author

F Solimene
Author
A Dello Russo
Author
C Tondo
Author
S Iacopino
Author
A Rossillo
Author
R Maggio
Author
S Themistoklakis
Author
M Bertini
Author
You may be interested in