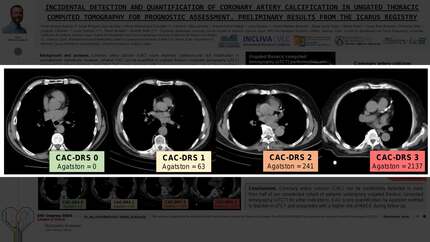
Incidental detection and quantification of coronary artery calcification in ungated thoracic computed tomography for prognostic assessment. Preliminary results from the ICARUS registry
European Heart Journal


Abstract
Coronary artery calcium (CAC) score improves cardiovascular risk stratification in asymptomatic individuals. However, whether CAC can be quantified in ungated thoracic computed tomography (uTCT) performed for other indications, and if this CAC score associates with cardiovascular outcomes, hasn’t been confirmed yet.
We aim to analyse the extension of CAC and its prognostic value in terms of major adverse cardiovascular events (MACE) in patients who underwent uTCT for other indications.
We analysed a preliminary sample of 115 uTCT performed in 2015 in our hospital. We studied the presence and extension of CAC and quantified the global CAC score by Agatston method using validated software. Patients were categorized according to Coronary Artery Calcium Data and Reporting System (CAC-DRS) categories. Cardiovascular risk factors, lipidic control and pharmacological therapy of the cohort were registered. We analysed the time to first 3P-MACE, defined as cardiovascular death, non-fatal myocardial infarction and non-fatal stroke, whichever occurred first. A p-value <0.05 was considered statistically significant.
Mean age of the cohort was 60.8±16.1 years (53% male, 53% smokers). Mean LDL-cholesterol was 121.67±34.91 mg/dL, and 35.1% received lipid-lowering therapy. In more than half (n=59, 51.3%) of the population CAC was detected. Mean CAC score was 312.99±774.48 Agatston units, and patients were categorized in CAC-DRS category 1 (n=19, 16.5%), category 2 (n=15, 13%) and category 3 (n=25, 21.7%). Patients with CAC were older (71±10.1 vs. 50.1±14.2 years, p<0.001), had higher burden of cardiovascular risk factors and prevalence of chronic kidney disease (CKD; n=8, 13.6% vs. n=1, 1.8%, p=0.03) and higher levels of triglycerides (143.2±80.5 vs. 106.8±36.2 mg/dL, p=0.004), but not LDL-cholesterol. Eleven (9.6%) patients presented 3P-MACE during a mean follow-up of 6.55±2.82 years. CAC score independently predicted 3P-MACE (HR 1.06 [1.01-1.11] per 100 Agatston units, p=0.02) along with CKD (HR 6.94 [1.58-30.46], p=0.01) and basal glucose levels (HR 1.03 [1.02-1.04] per mg/dL, p<0.001).
CAC can be incidentally detected in more than half of our unselected cohort of patients undergoing uTCT for other indications. CAC score quantification by Agatston method is feasible in uTCT and associates with a higher risk of MACE during follow-up. Incidental CAC detection in uTCT
Contributors


H Merenciano-Gonzalez
Author
C A Villa-Sanchez
Author
M Perez-Pelegri
Author
J Gavara
Author
C Bertolin-Boronat
Author
D Iraola-Viana
Author
N Perez
Author
C Rios-Navarro
Author
D Moratal
Author
You may be interested in