Feasibility and procedural safety of the pentaspline pulsed field ablation catheter for atrial lesions beyond pulmonary vein isolation
EP Europace Journal


Abstract
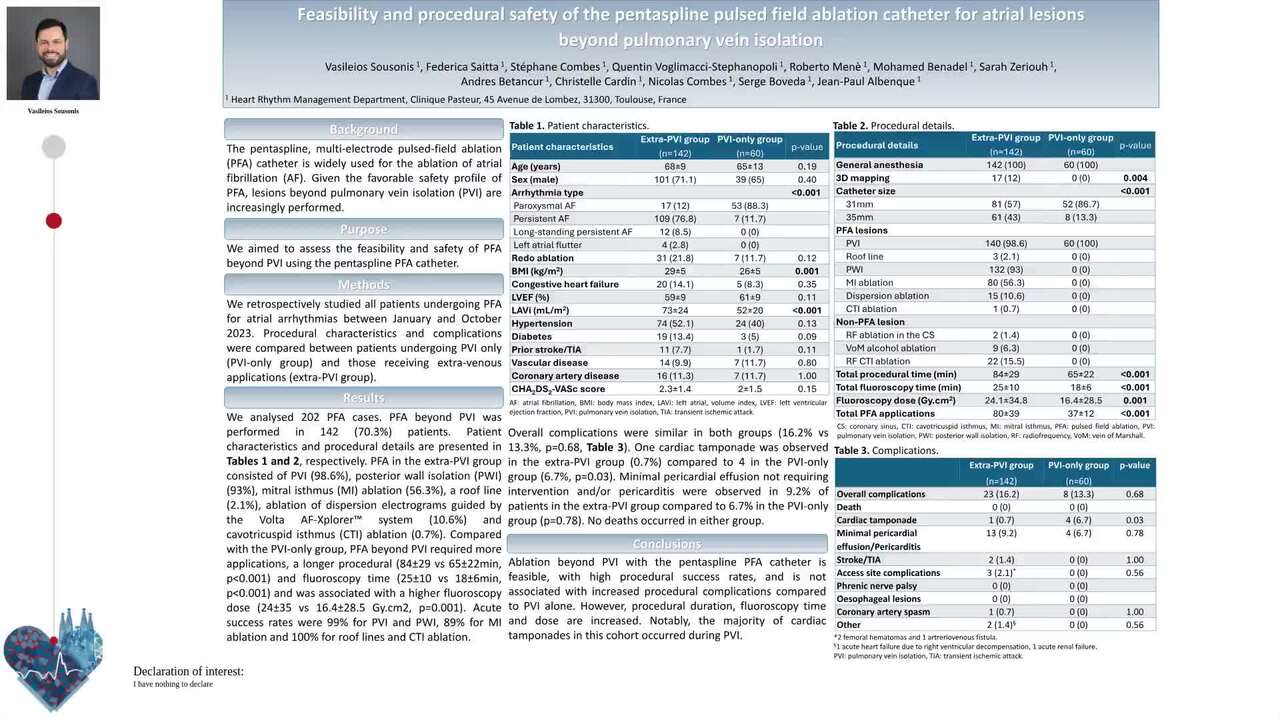
The pentaspline multi-electrode pulsed-field ablation (PFA) catheter is widely used for the ablation of atrial fibrillation (AF). Given the favorable safety profile of PFA, lesions beyond pulmonary vein isolation (PVI) are increasingly performed.
We aimed to assess the feasibility and safety of PFA beyond PVI with the pentaspline PFA catheter.
We retrospectively studied all patients who underwent PFA for atrial arrhythmias in our center between January and October 2023. Procedural characteristics and complications were compared between patients undergoing only PVI (PVI-only group) and those receiving extra-venous applications (extra-PVI group).
We analysed 202 PFA cases. Indications for ablation included paroxysmal AF (34.7%), persistent AF (57.4%), long-standing persistent AF (5.9%) and atypical atrial flutter (2%). Redo procedures accounted for 18.8% of the total cases. PFA beyond PVI was performed in 142 (70.3%) patients. Patients in the extra-PVI group had a higher incidence of persistent AF (76.8% vs 11.7%, p<0.001), a higher BMI (29±5 vs 26±5 kg/m2, p=0.001) and a more dilated left atrium (LAVI: 73±24 vs 52±20 ml/m2, p<0.001, Table 1). PFA in this group consisted of PVI (98.6%), posterior wall isolation (PWI) (93%), mitral isthmus (MI) ablation (56.3%), a roof line (2.1%), ablation of dispersion electrograms (10.6%) and cavotricuspid isthmus (CTI) ablation (0.7%). In 22 (15.5%) patients, additional CTI ablation with radiofrequency (RF) was performed, while alcohol ablation of the vein of Marshall and RF ablation in the coronary sinus were required in 9 (6.3%) and 2 (1.4%) patients, respectively, to achieve MI block.
Compared to the PVI-only group, PFA beyond PVI required a mean of 43 additional applications, a longer procedural (84±29 vs 65±22 min, p<0.001) and fluoroscopy time (25±10 vs 18±6 min, p<0.001) and had a higher fluoroscopy dose (24±35 vs 16.4±28.5 Gy.cm2, p=0.001). A three-dimensional electroanatomic map was used in 12% of cases. Acute success rates were 99% for PVI and PWI, 89% for MI ablation and 100% for roof lines and CTI ablation. Overall complication rates were similar in both groups (16.2% vs 13.3%, p=0.68, Table 2). One cardiac tamponade was observed in the extra-PVI group (0.7%) compared to 4 in the PVI-only group (6.7%, p=0.03). Among the latter, 2 incidents occurred during PVI in patients with long-standing persistent AF, precluding further extra-venous ablation. A small pericardial effusion (without hemodynamic compromise) and/or pericarditis were seen in 9.2% of patients in the extra-PVI group compared to 6.7% in the PVI-only group (p=0.78). No deaths occurred in either group.
Ablation beyond PVI with the pentaspline PFA catheter is feasible with high success rates and no apparent increase in procedural complications. However, it increases procedural duration and fluoroscopy. Notably, the majority of cardiac tamponades in this cohort occurred during PVI.
Contributors


Q Voglimacci-Stephanopoli
Author
R Mene
Author
M Benadel
Author
S Zeriouh
Author
Royal Papworth Hospital Cambridge , United Kingdom of Great Britain & Northern Ireland
A Betancur
Author
C Cardin
Author
N Combes
Author
S Boveda
Author
J P Albenque
Author
You may be interested in