Stereotactic arrhythmia radioablation for refractory ventricular tachycardia. A retrospective analysis and optimisation of the planning phase
EP Europace Journal


Abstract
Stereotactic arrhythmia radioablation (STAR) is used as a rescue treatment for refractory ventricular tachycardia (VT). However, the planning phase to accurately delineate the clinical target volume (CTV) still suffers from limitations due to the incompatibility of data formats between 3D electro-anatomical mapping systems (EAM) used for VT ablation and STAR planning software. The concordance between the CTVs as defined by the planning software (CTVSTAR) and the CTV based on EAM data (CTVEAM) remains unknown.
Within the STOPSTORM European consortium, we compared the concordance between CTVSTAR and CTVEAM in our series of 13 patients (pts) treated by STAR for refractory VT. We also evaluated need for redo ablation of VT after STAR.
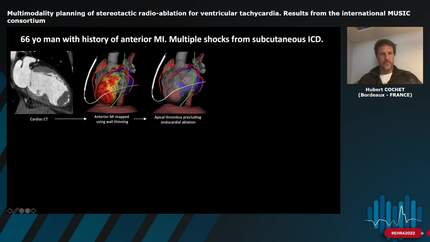
Using the software Slicer3D, two protocols were retrospectively compared: Protocol 1 comprised the manual contouring of the CTVSTAR based on 4D-CT SCAN drawn side-by-side using EAM (Carto3, Biosense Webster) screenshots and diagnostic reports. Protocol 2 comprised semiautomatic segmentation of CTVEAM based on 4D-CT SCAN using imported EAMs annotated with landmarks for VT substrate delimitation. The delineation of CTVEAM included 3 steps: (1) semiautomatic segmentation of ventricular myocardium (VM), the blood-pool of the concerned ventricle and at least 2 additional cardiac cavities; (2) 3D-alignment of EAM with the segmented cavities; and (3), 3D-delineation of CTVSTAR identified as the transmural section of VM segment surrounding the EAM’s VT substrate delimited by STAR tags (Figure 1). Volume overlap (Dice coefficient, 100% meaning complete overlap) and volume absolute difference (VAD, 0% meaning similar volumes) between CTVs were compared. The following cumulative averages were computed over time: redo ablation (RedoA) and CTV.
Figure 1 illustrates the last treated patient (#13) in whom the delineated volumes, CTVSTAR (red) and CTVEAM (blue), displayed good matching (Dice 72% and VAD 4. Figure 2 shows the comparison between CTVSTAR and CTVEAM for the 13 pts (65±7 yo) treated with STAR, resulting in a mean Dice of 47±17% and mean VAD of 40±51%. Figure 3 shows the cumulative RedoA and the cumulative averaged CTVSTAR and CTVEAM over time. Interestingly, the need for redo ablation decreased with increasing CTVs.
Our study demonstrates the efficacy of STAR treatment for refractory VT. Our confidence in STAR led to higher CTVs and lower RedoA over time. The high variability of CTV delineation using two different protocols suggests that STAR planning phase can be optimised by appointing intraprocedural anatomical landmarks to the VT substrate.
Contributors

A Luca
Author
C Herrera-Siklody
Author
M Van Der Ree
Author
P Postema
Author
C Teres
Author
M Le Bloa
Author
G Domenichini
Author
O Blanck
Author
J Verfhoff
Author
You may be interested in