Effects of diagnosis-to-ablation time and antiarrhythmic drug responsiveness on the rhythm outcomes of atrial fibrillation catheter ablation
EP Europace Journal


Abstract
Atrial fibrillation (AF) is a progressive disease. Additionally, delaying AF catheter ablation (AFCA) for a year, during antiarrhythmic drug (AAD) therapy does not reduce the efficacy of this ablation. This study explored AFCA rhythm outcomes based on the diagnosis-to-ablation time (DAT) and AAD responsiveness in participants with either paroxysmal AF (PAF) or persistent AF (PeAF).
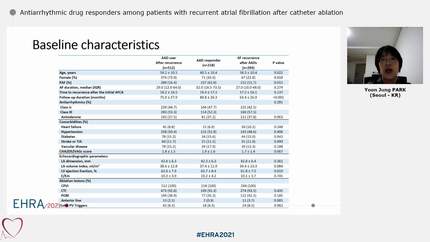
We included the data of 1,038 participants with AAD-resistant PeAF, all of whom had a clear time point for the diagnosis of PeAF and had undergone an AFCA for the first time. Participants who experienced recurrences of the paroxysmal type, while on AAD therapy, were analyzed as a cohort of AAD-partial-responders; whereas those who consistently maintained a PeAF, while on AAD therapy were analyzed as a cohort of AAD-non-responders. We calculated the DAT cutoff to determine long-term rhythm outcomes, using a maximum log-likelihood approach, based on the Cox proportional hazards regression model.
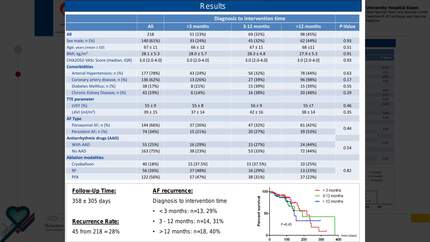
Of the participants, 79.8% were male, and the median age was 61 years. The cohort of AAD-non-responders had a higher body mass index and larger left atrial diameter than that of the cohort of AAD-partial-responders. Furthermore, the cohort of AAD-non-responders showed a significantly higher incidence of AF recurrence subsequent to AFCA (adjusted hazard ratio= 1.75, 95% confidence interval: 1.33–2.30; log-rank test: p< 0.001) than that of the cohort of AAD-partial-responders. The log-likelihood graphs of the Cox proportional hazards regression models showed bimodal morphology for the cutoff values of 22 and 40 months. The cutoff value of DAT that most optimally discriminated between rhythm outcomes was 22 months.
Thus, both the DAT and AAD responsiveness affected the rhythm outcomes of AFCA. Delaying AFCA to a DAT of longer than 22 months was inadvisable, particularly in the participants in whom PeAF progressed to PAF during AAD therapy.
Contributors

D H Kim
Author
Severance Cardiovascular Hospital, Yonsei University College of Medicine Seoul , Korea (Republic of)

K P Kim
Author
S H Choi
Author


J W Park
Author
Yonsei University College of Medicine, Yonsei University Health System Yongin , Korea (Republic of)
H T Yu
Author
Severance Cardiovascular Hospital, Yonsei University College of Medicine Seoul , Korea (Republic of)
T H Kim
Author
Severance Hospital, Yonsei University College of Medicine Seoul , Korea (Republic of)



You may be interested in