Cardiac perforation due to delayed migration of a chronic dialysis catheter: a case report
European Heart Journal - Case Reports


Abstract
Tunnelled haemodialysis catheters are commonly used to perform haemodialysis. Rare complications of these catheters include perforations of major blood vessels or the heart. Albeit rare, these complications can lead to significant morbidity and mortality.
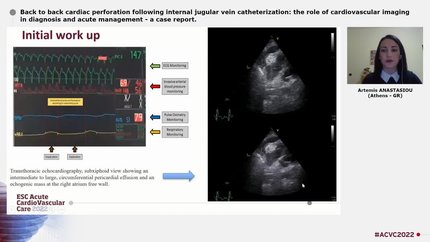
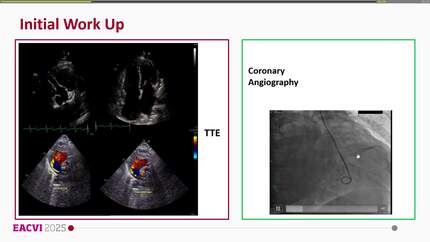
We present a case of late migration of a tunnelled haemodialysis catheter causing a right atrial perforation with subsequent pericardial tamponade, haemodynamic shock, and cardiac arrest. A 51-year-old female patient with end-stage renal disease presented with hypotension and lactate acidosis, indicating circulatory shock, during ambulatory intermittent haemodialysis. Dialysis was performed through a tunnelled haemodialysis catheter that had been implanted more than 1 year ago. Upon admission to the hospital, initial diagnostics, including transthoracic echocardiography and computed tomography scan, showed a circumferential pericardial effusion which was not haemodynamically significant and no other pathological findings. After being transferred to the intensive care unit, the patient again showed signs of haemodynamic shock at the start of another dialysis session which deteriorated to cardiac arrest. Ultimately, using multi-modality imaging, migration of the catheter tip through the right atrial wall into the pericardial space was diagnosed. Emergency sternotomy and surgical extraction of the tunnelled haemodialysis catheter were performed and the patient recovered completely.
Migration and perforation of a tunnelled haemodialysis catheter can occur late after implantation and lead to circulatory shock, thus requiring immediate diagnostic workup and surgical therapy. Routine diagnostic procedures may be insufficient for making a correct diagnosis. More specific approaches, such as multi-modality imaging including contrast echocardiography, should be implemented upon clinical suspicion.
Contributors

Elion Hoxha
Author
Gerold Söffker
Author

Soren Skott-Schmiegelow
Author
Poonam Velagapudi
Author
Christoph Vandenbriele
Author
Vincenzo Nuzzi
Author
Reshma Amin
Author
Deepti Ranganathan
Author
You may be interested in