Transcatheter versus surgical aortic valve replacement in lower-risk and higher-risk patients: a meta-analysis of randomized trials
European Heart Journal


Abstract
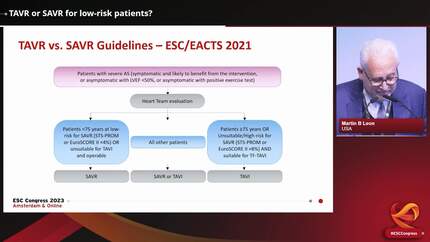
Additional randomized clinical trial (RCT) data comparing transcatheter aortic valve implantation (TAVI) with surgical aortic valve replacement (SAVR) is available, including longer term follow-up. A meta-analysis comparing TAVI to SAVR was performed. A pragmatic risk classification was applied, partitioning lower-risk and higher-risk patients.
The main endpoints were death, strokes, and the composite of death or disabling stroke, occurring at 1 year (early) or after 1 year (later). A random-effects meta-analysis was performed. Eight RCTs with 8698 patients were included. In lower-risk patients, at 1 year, the risk of death was lower after TAVI compared with SAVR [relative risk (RR) 0.67; 95% confidence interval (CI) 0.47 to 0.96,
In lower-risk patients, there was an early mortality reduction with TAVI, but no differences after later follow-up. There was also an early reduction in the composite of death or disabling stroke, with no difference at later follow-up. There were no significant differences for higher-risk patients. Informed therapy decisions may be more dependent on the temporality of events or secondary endpoints than the long-term occurrence of main clinical outcomes.
Contributors

Yousif Ahmad
Author
James P Howard
Author

Ahran D Arnold
Author
Imperial College London London , United Kingdom of Great Britain & Northern Ireland
Mahesh V Madhavan
Author
Christopher M Cook
Author
Maria Alu
Author
Michael J Mack
Author
Michael J Reardon
Author
Vinod H Thourani
Author
Samir Kapadia
Author
Hans Gustav Hørsted Thyregod
Author
Lars Sondergaard
Author
Troels Højsgaard Jørgensen
Author
William D Toff
Author
University of Leicester Leicester , United Kingdom of Great Britain & Northern Ireland
Nicolas M Van Mieghem
Author
Raj R Makkar
Author
John K Forrest
Author
Martin B Leon
Author
You may be interested in