Coronary computed tomography angiography vs. myocardial single photon emission computed tomography in patients with intermediate risk chest pain: a randomized clinical trial for cost-effectiveness comparison based on real-world cost
European Heart Journal - Cardiovascular Imaging


Abstract
To compare the cost-effectiveness of coronary computed tomography angiography (CCTA) vs. myocardial single photon emission computed tomography (SPECT) in patients with stable intermediate risk chest pain.
Non-acute patients with 10–90% pre-test probability of coronary artery disease from three high-volume centres in Korea (
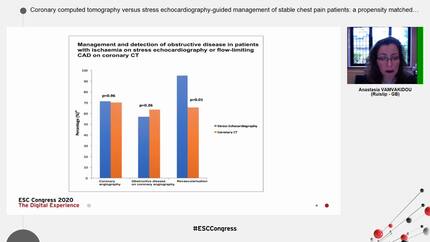
CCTA is associated with fewer subsequent ICA with no difference in downstream outcome. CCTA may be more cost-effective than SPECT in Korean patients with stable, intermediate risk chest pain.
Contributors

Seung-Pyo Lee
Author
Jae-Kyung Seo
Author
In-Chang Hwang
Author
Jun-Bean Park
Author
Eun-Ah Park
Author
Whal Lee
Author
Jin-Chul Paeng
Author
Hyun-Ju Lee
Author
Yeonyee E Yoon
Author
Hack-Lyoung Kim
Author
Eunbee Koh
Author
Insun Choi
Author
Ji Eun Choi
Author

You may be interested in